


 Sign Out
Sign Out
The prescribed dose should be administered orally with a meal and a large glass of water to minimise the risk of gastrointestinal irritations. Doses of 400 mg or 600 mg should be administered once daily, whereas a daily dose of 800 mg should be administered as 400 mg twice a day, in the morning and in the evening. For patients (children) unable to swallow the capsules the content of may be diluted in a glass of still water or apple juice.
Since studies in animals have shown reproductive toxicity, and the potential risk for the human foetus in unknown, women of child-bearing potential who open capsules should be advised to handle the contents with caution and avoid skin-eye contact or inhalation. Hands should be washed immediately after handling open capsules.
Posology for CML in adult patients: The recommended dosage of Imatinib is 400 mg/day for adult patients in chronic phase CML. Chronic phase CML is defined when all of the following criteria are met: blasts <15% in blood and bone marrow, peripheral blood basophils <20%, platelets >100 x 109/L.
The recommended dosage of Imatinib is 600 mg/day for adult patients in accelerated phase. Accelerated phase is defined by the presence of any of the following: blasts ≥15% but <30% in blood or bone marrow, blasts plus promyelocytes ≥30% in blood or bone marrow (providing <30% blasts), peripheral blood basophils ≥20%, platelets <100 x 109/L unrelated to therapy.
The recommended dose of Imatinib is 600 mg/day for adult patients in blast crisis. Blast crisis is defined as blasts ≥30% in blood or bone marrow or extramedullary disease other than hepatosplenomegaly.
Treatment duration: In clinical trials, treatment with Imatinib was continued until disease progression. The effect of stopping treatment after the achievement of a complete cytogenetic response has not been investigated.
Dose increases from 400 mg to 600 mg or 800 mg in patients with chronic phase disease, or from 600 mg to a maximum of 800 mg (given as 400 mg twice daily) in patients with accelerated phase or blast crisis may be considered in the absence of severe adverse drug reaction and severe non-leukaemia-related neutropenia or thrombocytopenia in the following circumstances: disease progression (at any time); failure to achieve a satisfactory haematological response after at least 3 months of treatment; failure to achieve a cytogenetic response after 12 months of treatment; or loss of a previously achieved haematological and/or cytogenetic response. Patients should be monitored closely following dose escalation given the potential for an increased incidence of adverse reactions at higher dosages.
Posology for CML in children: Dosing for children should be on the basis of body surface area (mg/m2). The dose of 340 mg/m2 daily is recommended for children with chronic phase CML and advanced phase CML (not to exceed the total dose of 800 mg). Treatment can be given as a once daily dose or alternatively the daily dose may be split into two administrations - one in the morning and one in the evening. The dose recommendation is currently based on a small number of paediatric patients. There is no experience with the treatment of children below 2 years of age.
Dose increases from 340 mg/m2 daily to 570 mg/m2 daily (not to exceed the total dose of 800 mg) may be considered in children in the absence of severe adverse drug reaction and severe non-leukaemia-related neutropenia or thrombocytopenia in the following circumstances: disease progression (at any time); failure to achieve a satisfactory haematological response after at least 3 months of treatment; failure to achieve a cytogenetic response after 12 months of treatment; or loss of a previously achieved haematological and/or cytogenetic response. Patients should be monitored closely following dose escalation given the potential for an increased incidence of adverse reactions at higher dosages.
Posology for Ph+ ALL in adult patients: The recommended dose of Imatinib is 600 mg/day for adult patients with Ph+ ALL. Haematological experts in the management of this disease should supervise the therapy throughout all phases of care.
Treatment schedule: On the basis of the existing data, Imatinib has been shown to be effective and safe when administered at 600 mg/day in combination with chemotherapy in the induction phase, the consolidation and maintenance phases of chemotherapy for adult patients with newly diagnosed Ph+ ALL. The duration of Imatinib therapy can vary with the treatment programme selected, but generally longer exposures to Imatinib have yielded better results.
For adult patients with relapsed or refractory Ph+ALL Imatinib monotherapy at 600 mg/day is safe, effective and can be given until disease progression occurs.
Posology for Ph+ ALL in children: Dosing for children should be on the basis of body surface area (mg/m2). The dose of 340 mg/m2 daily is recommended for children with Ph+ ALL (not to exceed the total dose of 600 mg).
Posology for MDS/MPD: The recommended dose of Imatinib is 400 mg/day for adult patients with MDS/MPD.
Treatment duration: In the only clinical trial performed up to now, treatment with Imatinib was continued until disease progression. At the time of analysis, the treatment duration was a median of 47 months (24 days - 60 months).
Posology for HES/CEL: The recommended dose of Imatinib is 100 mg/day for adult patients with HES/CEL.
Dose increase from 100 mg to 400 mg may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy. Treatment should be continued as long as the patient continues to benefit.
Posology for GIST: The recommended dose of Imatinib is 400 mg/day for adult patients with unresectable and/or metastatic malignant GIST.
Limited data exist on the effect of dose increases from 400 mg to 600 mg or 800 mg in patients progressing at the lower dose.
Treatment duration: In clinical trials in GIST patients, treatment with Imatinib was continued until disease progression. At the time of analysis, the treatment duration was a median of 7 months (7 days to 13 months). The effect of stopping treatment after achieving a response has not been investigated.
The recommended dose of Imatinib is 400 mg/day for the adjuvant treatment of adult patients following resection of GIST. Optimal treatment duration is not yet established. Length of treatment in the clinical trial supporting this indication was 36 months.
Posology for DFSP: The recommended dose of Imatinib is 800 mg/day for adult patients with DFSP.
Dose adjustment for adverse reactions: Non-haematological adverse reactions: If a severe non-haematological adverse reaction develops with Imatinib use, treatment must be withheld until the event has resolved. Thereafter, treatment can be resumed as appropriate depending on the initial severity of the event.
If elevations in bilirubin >3 x institutional upper limit of normal (IULN) or in liver transaminases >5 x IULN occur, Imatinib should be withheld until bilirubin levels have returned to <1.5 x IULN and transaminase levels to <2.5 x IULN. Treatment with Imatinib may then be continued at a reduced daily dose. In adults the dose should be reduced from 400 to 300 mg or from 600 to 400 mg, or from 800 mg to 600 mg, and in children from 340 to 260 mg/m2/day.
Haematological adverse reactions: Dose reduction or treatment interruption for severe neutropenia and thrombocytopenia are recommended as indicated in the table as follows. Dose adjustments for neutropenia and thrombocytopenia: See Table 1.
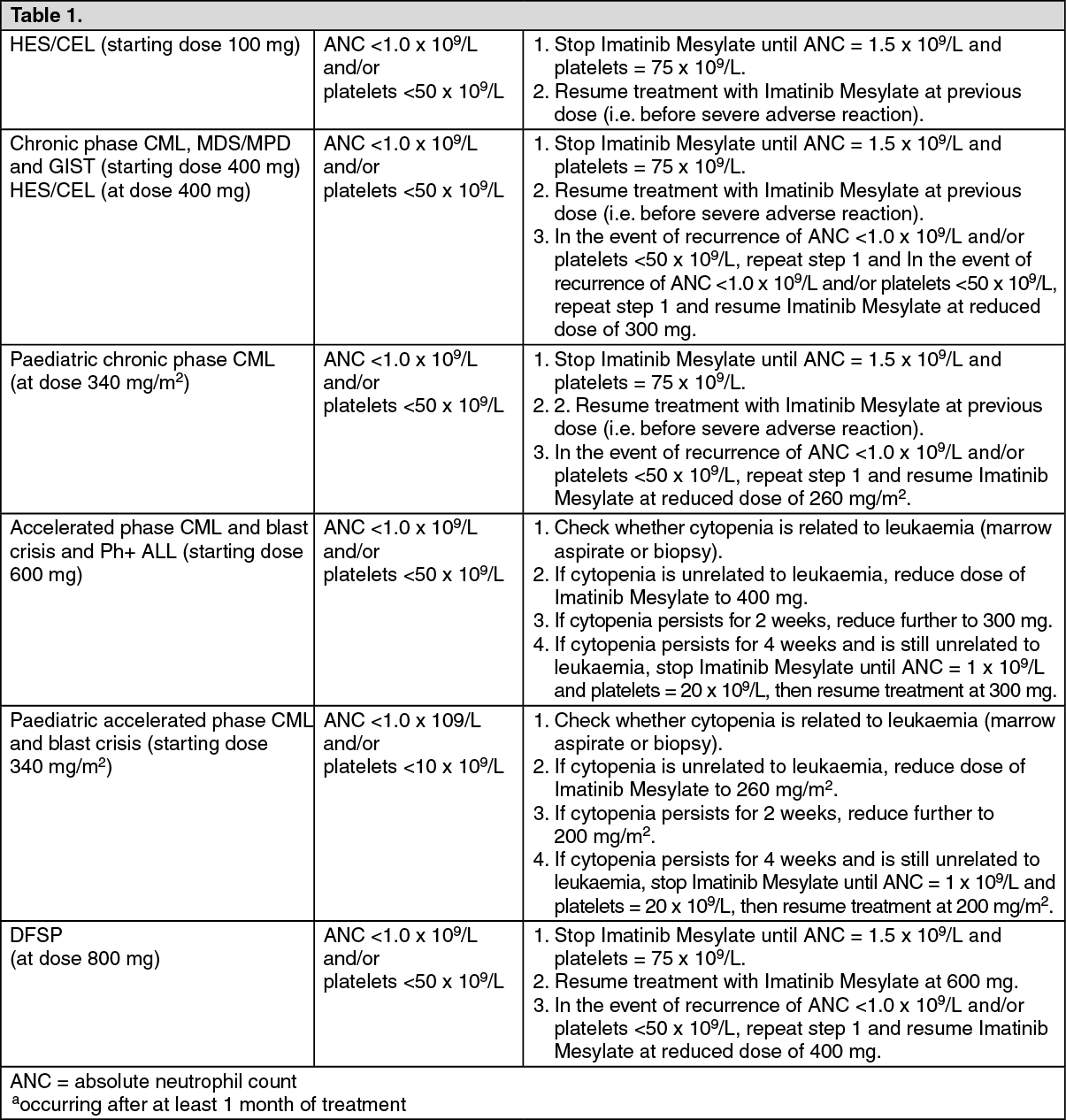 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial populations: Paediatric use: There is no experience in children with CML below 2 years of age and with Ph+ALL below 1 year of age.
There is very limited experience in children with MDS/MPD, DFSP, GIST and HES/CEL.
The safety and efficacy of imatinib in children with MDS/MPD, DFSP, GIST and HES/CEL aged less than 18 years of age have not been established in clinical trials. Currently available published data are summarised in Pharmacology: Pharmacodynamics under Actions but no recommendation on a posology can be made.
Hepatic insufficiency: Imatinib is mainly metabolised through the liver. Patients with mild, moderate or severe liver dysfunction should be given the minimum recommended dose of 400 mg daily. The dose can be reduced if not tolerated.
Liver dysfunction classification: See Table 2.
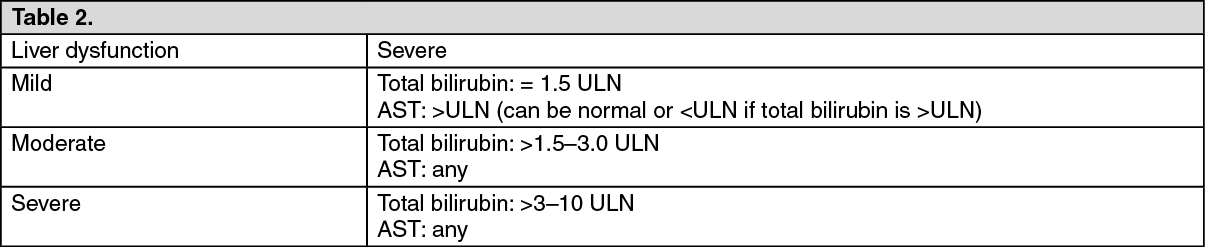 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRenal insufficiency: Patients with renal dysfunction or on dialysis should be given the minimum recommended dose of 400 mg daily as starting dose. However, in these patients caution is recommended. The dose can be reduced if not tolerated. If tolerated, the dose can be increased for lack of efficacy.
Older people: Imatinib pharmacokinetics have not been specifically studied in older people. No significant age-related pharmacokinetic differences have been observed in adult patients in clinical trials which included over 20% of patients age 65 and older. No specific dose recommendation is necessary in older people.